
Cortisol Isn’t the Problem. This Is.
Learn how cortisol should work, what happens when stress flattens your daily rhythm, and the evidence-based protocol to reset it.

Cortisol has developed a reputation in wellness culture as the villain of modern life, something to suppress or detox. This is precisely the wrong frame.
Cortisol is not a toxin. It’s one of the most precisely designed survival hormones in human biology. Its job, when working correctly, is essential. The problem is not cortisol itself, but a system that cannot turn off.
Every morning, roughly 20-30 minutes after you wake up, your cortisol levels surge 50-160% above their overnight lows. This is the cortisol awakening response (CAR) — a deliberate, adaptive biological signal that does several necessary things simultaneously.
It mobilizes glucose from the liver, giving your brain and muscles an energy substrate before you have eaten. It sharpens cognitive focus, improving the speed and accuracy of early-morning decisions. It modulates the immune system, briefly suppressing inflammation to allow the body to redirect resources toward activity. It coordinates with your circadian clock to synchronize dozens of other hormonal and metabolic signals.
By midday, cortisol should be declining. By evening, it should be approaching its daily minimum. By the time you sleep, it should be low enough to allow slow-wave sleep and the biological repair processes that depend on it.
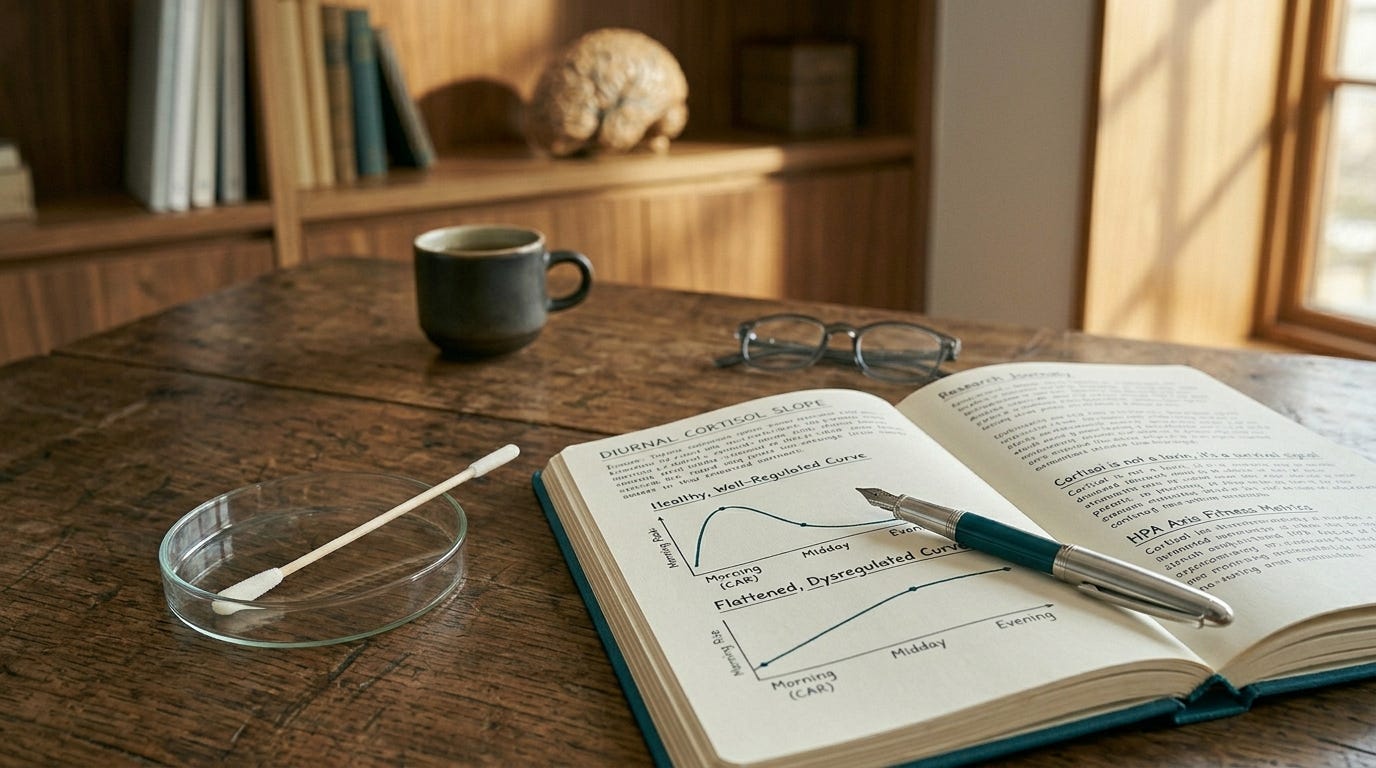
This curve — steep in the morning, declining through the day, low by night — is the signature of a well-regulated HPA axis. It’s the pattern that research consistently associates with lower inflammatory markers, better metabolic health, clearer cognition, and longer life.¹
The problem begins when the curve flattens.
What Happens When the System Cannot Turn Off
Chronic stress — occupational, relational, financial, physical, or any sustained demand that outpaces recovery — disrupts the negative feedback loop that should turn cortisol off once the stressor has passed.¹ The result is a system in which cortisol is sometimes too high at the wrong times, sometimes too low at the wrong times, and almost always dysregulated in its daily rhythm.
The downstream consequences of this dysregulation reach every major organ system in the body. Here is what the evidence documents.
Visceral fat accumulation. Visceral adipose tissue contains approximately four times more glucocorticoid receptors than subcutaneous fat. When cortisol is chronically elevated, it preferentially deposits fat deep in the abdomen — not as a cosmetic problem, but as a metabolic one. Visceral fat is the most pro-inflammatory fat depot in the body, releasing cytokines that further dysregulate the HPA axis. The cycle feeds itself.¹ Cushing’s syndrome — the condition caused by pathologically elevated cortisol — provides the clearest demonstration: virtually every Cushing’s patient develops central obesity, regardless of caloric intake.
Thyroid conversion block. The thyroid gland produces mostly T4, an inactive precursor. T4 must be converted to T3 — the active form — by deiodinase enzymes primarily in the liver and kidney. Cortisol suppresses the activity of 5’-deiodinase, the enzyme responsible for this conversion. Under chronic stress, T4 is redirected away from active T3 and toward reverse T3, an inactive hormone that competes with T3 for receptor binding.¹ The result is a functional hypothyroid state: fatigue, slowed metabolism, cold intolerance, low mood, difficulty concentrating — with a TSH that looks completely normal, because the problem is in the conversion, not in the thyroid’s production.
Insulin resistance. Cortisol raises blood glucose by stimulating hepatic glucose production and reducing insulin sensitivity in peripheral tissues. This is adaptive in acute stress — you need available glucose to fight or flee. Chronically, it’s destructive. Sustained cortisol elevation keeps blood glucose elevated, demands more insulin from the pancreas, and progressively reduces the sensitivity of glucose transporters.¹ Insulin resistance, visceral fat, and HPA dysregulation form a mutually reinforcing triad that is very difficult to interrupt from any single point.
Sleep architecture destruction. Cortisol and slow-wave sleep are directly antagonistic: deep sleep suppresses cortisol; cortisol suppresses deep sleep. When evening cortisol is elevated, slow-wave sleep is compressed. The overnight repair processes that depend on it — cellular maintenance, glymphatic clearance, immune consolidation, NAD+ restoration — are shortened.¹ The 3am waking pattern is the clinical signature of this: cortisol begins its morning ascent too early, crossing the threshold that triggers wakefulness before the biological morning has arrived.
Hippocampal damage. The hippocampus is the brain’s primary hub for memory encoding, emotional regulation, and context processing. It also has the highest density of glucocorticoid receptors of any brain structure — which means it’s both cortisol’s most important target and its most vulnerable victim. Prolonged cortisol elevation causes hippocampal neuronal atrophy, reduces the production of BDNF (the growth factor that maintains neuronal health), and impairs the hippocampal regulation of the HPA axis itself.¹ The result is a self-amplifying loop: stress damages the very brain region responsible for moderating the stress response.
Immune dysregulation. Acute cortisol is powerfully anti-inflammatory — it’s why synthetic glucocorticoids like prednisone are used to treat inflammatory conditions. Chronic cortisol, however, produces glucocorticoid receptor resistance: the immune system becomes desensitized to cortisol’s anti-inflammatory signals while remaining activated by other inflammatory triggers.¹ The paradox is that chronically stressed people are simultaneously cortisol-saturated and more inflamed than their unstressed counterparts — the system that was designed to suppress inflammation has lost its ability to do so effectively.
What a Standard Cortisol Test Cannot Tell You
A single morning blood cortisol measurement — which is the extent of cortisol assessment in standard primary care — tells you almost nothing useful about HPA axis function. It captures one point on a curve that should be dynamic, rhythmic, and context-dependent.
What actually matters is the shape of the diurnal cortisol profile: how steep is the morning rise, how rapidly does it decline through the day, and how low does it reach by evening. A flattened slope — where morning cortisol is lower than it should be and evening cortisol higher than it should be — is the biological signature of chronic stress and burnout, and it’s one of the most consistent predictors of adverse health outcomes in the longitudinal cortisol literature.¹
The most accessible clinical assessment is the cortisol awakening response test — saliva samples collected immediately upon waking, 15 minutes after waking, and 30 minutes after waking. This is available through home collection kits and several functional medicine laboratories. It’s not available on a standard GP or internist panel, and this is a significant gap in routine preventive assessment.
The DUTCH test (Dried Urine Test for Comprehensive Hormones), provides a full diurnal cortisol curve, cortisol metabolites, and the HPA axis markers that reveal whether the system is compensating, depleted, or hyperactivated. It’s the most comprehensive non-invasive assessment of cortisol dynamics currently available to consumers.
The paid section covers what the evidence actually supports for resetting the HPA axis — with specific doses, specific formats, and the crucial nuances that most content on this topic misses entirely. Including the exercise finding that directly contradicts what most people believe about stress and physical intensity, the ashwagandha data that shows something important that most ashwagandha advocates don’t mention, and the sleep intervention that has a larger effect on cortisol regulation than any supplement in the literature.